
What Is Manual FUE and How Does It Work?
Manual FUE removes individual hair follicles by hand using a small punch tool. A surgeon extracts each graft personally without machines.
Manual FUE stands for Manual Follicular Unit Extraction. This technique removes hair graftsA hair graft refers to a small unit of hair-bearing skin taken from the donor area—typically the back or sides... one by one from the donor areaThe Source of Restoration The donor area plays a critical role in hair transplantation, as it serves as the source.... A surgeon uses a handheld punch tool. The tool measures between 0.7 mm and 1.0 mm in diameter. The surgeon rotates this tool by hand. This rotation cuts around each follicular unit. Then the surgeon pulls out the graft with forceps.
This method differs from older techniques. Strip surgery (FUT) removed a whole strip of scalp. That method left a linear scar. FUE changed everything. Surgeons began extracting individual grafts instead. This left tiny dot scars only. Patients healed faster. They also wore short hair without visible scars.
Hair transplantationHair transplantation is a surgical procedure that involves the extraction of hair follicles from a designated donor site, followed by... evolved over decades. Doctors first used large plugs in the 1950s. These looked unnatural. Then came mini-grafts and micro-grafts. FUT arrived in the 1990s. FUE followed in the early 2000s. Now surgeons choose between manual FUE, motorized FUE, and robotic FUE. Each version serves different needs.
Manual FUE holds strong clinical relevance today. Many top surgeons prefer it for hairline work. The hand control gives better precision. The surgeon feels each graft. This tactile feedback matters greatly. It helps the surgeon avoid damage. It also helps place grafts at perfect angles.
|
Technique |
Scar Type |
Healing Time |
Control Level |
|
FUT (Strip) |
Linear scar |
2-3 weeks |
Moderate |
|
Motorized FUE |
Dot scars |
1-2 weeks |
Good |
|
Manual FUE |
Micro-dot scars |
5-10 days |
Excellent |
|
Robotic FUE |
Dot scars |
1-2 weeks |
Automated |
Manual FUE prioritizes precision over speed. Motorized tools work faster. Robots work consistently. But manual work gives the surgeon direct contact with each graft. This matters for quality. Studies show that surgeon skill affects outcomes more than tool type (Unger and Shapiro, 2019).
What Are the Scientific Principles Behind FUE?

FUE works because hair follicles live in natural groups. Surgeons move these groups from donor areas to bald areas. The follicles keep growing in their new location.
How Do Follicular Units Structure Human Hair?
Follicular units contain 1 to 4 hairs growing together in a small bundle. These bundles share blood supply and nerves.
Human scalp hair grows in natural groupings. Researchers call these groupings follicular units. Each unit contains one to four terminal hairs. It also contains one or two vellus hairs. Sebaceous glands sit nearby. Small muscles and nerves connect to the unit. A collagenA structural protein found in the skin and other connective tissues, which is responsible for skin firmness and elasticity.... band wraps around the whole group.
This structure matters for extraction. The punch tool must encircle this entire unit. If the punch cuts through the unit, hairs die. If the punch misses hairs, grafts become incomplete. Surgeons study these units under magnification before surgery.
Donor dominance theory explains why transplanted hair grows permanently. This theory states that hair follicles keep their original characteristics after moving. Donor area hair resists balding hormones. When surgeons move this hair to bald areas, it keeps growing. It does not fall out like the original hair did. Bernstein and Rassman (2006) confirmed this principle through long-term studies.
What Are the Core Steps of FUE Surgery?
FUE involves two main steps. First, the surgeon separates grafts from surrounding skin. Second, the surgeon pulls out and implants these grafts.
Step one requires isolation. The surgeon places the punch around a follicular unit. The punch cuts through skin and fat. It reaches the depth of the hair roots. The surgeon rotates the punch carefully. This rotation severs connective tissue. But it must not cut the graft itself.
Step two requires extraction. The surgeon uses fine forceps. The forceps grip the graft gently. The surgeon pulls upward with steady pressure. The graft slides out intact. Then technicians place it in preservation solution. This solution keeps the graft alive.
Implantation forms the final step. The surgeon makes tiny cuts in the recipient area. These cuts match the graft size. The surgeon inserts each graft into these cuts. The angle and direction must match natural hair flow. This creates undetectable results.
What Makes Manual FUE Different From Other Methods?
Manual FUE uses only hand-powered tools. No motors. No robots. The surgeon controls every movement through direct touch.
How Does the Manual Technique Actually Function?
A surgeon holds a sharp metal punch. The surgeon twists this punch between thumb and finger. This hand rotation cuts around each graft.
The manual punch looks simple. It resembles a small pen with a circular blade at the tip. But this simplicity hides great skill. The surgeon must control depth exactly. Too shallow cuts miss the graft. Too deep cuts damage underlying tissue. The surgeon feels resistance through the tool. This tactile feedback guides proper depth.
Hand-controlled rotation differs from motorized rotation. Motors spin at fixed speeds. Hands vary speed naturally. The surgeon slows down around curved hairs. The surgeon speeds up on straight hairs. This adaptability protects grafts.
No machine assists the surgeon. The surgeon provides all power and control. This demands excellent hand-eye coordination. It also demands physical endurance. A typical case requires thousands of these hand rotations.
What Is the Complete Manual FUE Workflow?
The workflow includes seven stages. Preparation, anesthesiaEnsuring Comfort During Hair Transplants Sedation is used in hair transplantation to help patients remain calm and comfortable throughout the..., extraction, preservation, site creation, implantation, and postoperative care.
First, the team prepares the donor area. Usually this means the back or sides of the head. They trim hair short. This exposes the scalp. Then they mark the extraction zone.
Second, the surgeon applies local anesthesia. Numbing medicine removes pain. The patient stays awake. They feel pressure but no sharp pain.
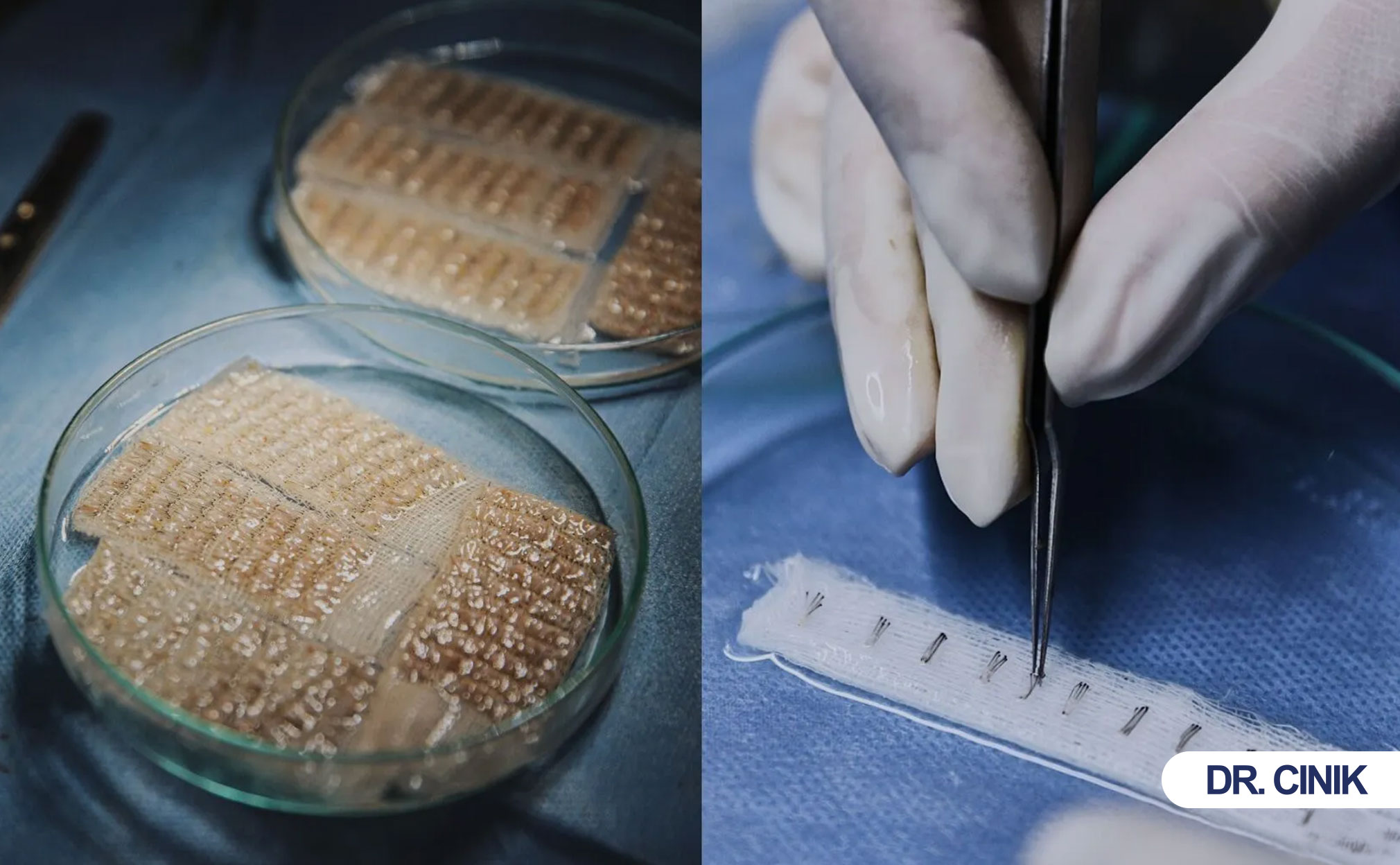
Third, extraction begins. The surgeon works methodically. They extract grafts row by row. Technicians sort grafts by hair count. They place grafts in chilled saline solution. This cold storage keeps cells alive.
Fourth, preservation continues throughout surgery. Technicians monitor temperature. They check graft hydration. Time outside the body affects survival. Teams work efficiently to minimize this time.
Fifth, the surgeon creates recipient sites. They use blades or needles. These make tiny slits in bald areas. The pattern follows natural hair direction.
Sixth, implantation occurs. Technicians or surgeons place grafts into sites. They match graft size to site size. They control angle carefully.
Seventh, postoperative care begins immediately. The team provides instructions. They schedule follow-up visits.
What Advantages Does Manual FUE Offer?

Manual FUE gives surgeons direct touch control. This reduces graft damage. It improves natural results. It also speeds patient healing.
How Does Surgical Precision Improve With Manual Control?
Direct tactile feedback lets surgeons feel each graft. They adjust angle and depth instantly. This reduces mistakes.
Surgeons using manual tools feel everything. They feel when the punch meets resistance. They feel when the graft releases. This sensory information guides decisions. Motorized tools block this feedback. The motor vibration hides subtle sensations.
This precision improves angle accuracy. Hair grows at specific angles under the skin. The punch must follow this angle. Manual control lets the surgeon curve the punch path. They follow the natural hair trajectory. This reduces transection rates.
Transection means cutting through a hair follicleA hair follicle is a small, tube-like structure embedded in the scalp that produces and grows individual strands of hair..... A transected graft dies. Studies show that experienced manual surgeons achieve transection rates below 5% (Parsley and Lam, 2018). Some motorized systems show higher rates. The surgeon’s skill matters more than the tool.
Why Does Graft Survival Increase With Manual Extraction?
Manual tools create less mechanical trauma. They produce no heat. They generate no friction. Grafts stay healthier.
Motorized punches spin rapidly. This spinning creates heat through friction. Heat damages delicate follicle cells. Manual rotation stays cool. The slow hand movement produces minimal friction.
Mechanical trauma also differs. Motors pull grafts with consistent force. Sometimes this force proves too strong. It strips protective tissue from the graft. Manual force varies. The surgeon eases pressure on fragile grafts. They increase pressure on tough grafts.
Graft quality directly affects results. High-quality grafts contain intact follicles. They include surrounding protective tissue. They show no crush injuries. Manual extraction preserves these features better.
How Do Aesthetic Outcomes Improve?
Manual control helps surgeons design better hairlines. They place grafts at exact angles. This creates natural-looking density.
Hairline design requires artistry. The surgeon must recreate natural patterns. Single-hair grafts belong at the front edge. Multi-hair grafts fill behind them. The transition must look gradual.
Manual implantation gives better control. The surgeon feels the site depth. They place grafts at the perfect level. Too deep creates pitting. Too shallow creates cobblestoning. Manual touch finds the middle ground.
Density planning also improves. Surgeons can pack grafts closer manually. They control spacing exactly. This creates fuller appearance without damaging blood supply.
How Does Patient Recovery Compare?
Manual FUE leaves smaller wounds. These heal faster. Patients return to normal activities sooner.
Manual punches often use smaller diameters. Some measure just 0.7 mm. Motorized systems sometimes need larger punches. Smaller holes heal quicker. They also scar less.
The extraction process causes less tissue disruption manually. The surgeon removes only necessary tissue. They avoid the “tenting” effect some motors cause. This preserves more donor area for future use.
Patients report less postoperative discomfort. The gentle manual extraction reduces inflammation. Swelling decreases faster. Redness fades within days rather than weeks.
|
Advantage |
Manual FUE |
Motorized FUE |
|
Transection Rate |
3-5% |
5-10% |
|
Heat Generation |
None |
Present |
|
Tactile Feedback |
Full |
Limited |
|
Hairline Precision |
Excellent |
Good |
|
Healing Time |
5-7 days |
7-10 days |
|
Donor Scarring |
Minimal |
Minimal to Moderate |
What Limitations and Challenges Does Manual FUE Face?
Manual FUE takes longer. It tires surgeons. It limits daily graft numbers. Results depend heavily on surgeon skill.
Why Does Procedure Duration Increase?
Hand extraction moves slowly. A surgeon extracts each graft individually. A typical session lasts 6 to 9 hours.
Motorized tools extract grafts in seconds. Manual extraction takes longer per graft. The surgeon must position, rotate, and remove each graft carefully. This careful pace protects quality. But it extends surgery time.
A 2000-graft case might take 8 hours manually. The same case might take 4 hours motorized. Patients must prepare for longer sessions. They need patience. They also need comfortable positioning during surgery.
How Does Surgeon Dependency Affect Outcomes?
Manual FUE requires expert hands. Results vary greatly between surgeons. Patients must choose experienced doctors.
This technique demands years of practice. New surgeons struggle with depth control. They may transect many grafts. They may extract grafts incompletely. Experience reduces these errors.
Endurance matters too. Surgeons perform thousands of repetitive motions. Fatigue sets in after hours. A tired surgeon makes more mistakes. The best surgeons maintain concentration throughout long cases.
Skill variation creates outcome differences. One surgeon may achieve 95% graft survival. Another may achieve only 80%. Patients should research surgeon experience carefully. They should ask about manual case numbers.
What Physical Constraints Limit Manual FUE?
Surgeon fatigue affects consistency. Long cases limit graft totals. Very large cases may need multiple sessions.
Human hands tire. Fingers cramp. Wrists ache. These physical limits affect performance. After 6 hours, speed and accuracy may drop. Surgeons recognize this. They schedule breaks. They also limit daily graft numbers.
Most manual surgeons extract 1500 to 2500 grafts per day. Some motorized teams extract 4000 grafts. This difference matters for advanced baldness. Severe hair loss needs many grafts. Manual FUE may require multiple sessions.
Physical constraints also affect consistency. The first 500 grafts may show perfect technique. The last 500 may show slight variation. Teams monitor quality throughout the day. They adjust pace as needed.
How Does Manual FUE Compare to Motorized and Robotic Methods?
Manual FUE gives best precision. Motorized FUE gives best speed. Robotic FUE gives best consistency. Each serves different needs.
What Are the Key Differences Between These Methods?
Manual uses hand power. Motorized uses electric power. Robotic uses computer guidance. Each changes the extraction experience.
Manual FUE relies entirely on surgeon skill. The surgeon provides motion, pressure, and judgment. No external power assists. This creates maximum adaptability. The surgeon changes technique instantly for each graft.
Motorized FUE uses electric or pneumatic motors. These spin the punch automatically. The surgeon guides the tool. The motor provides rotation. This speeds extraction. But it reduces tactile feedback. It also introduces heat and vibration.
Robotic FUE uses artificial intelligence. Cameras map the scalp. Computers identify grafts. Robotic arms extract them. This reduces human error. But it limits artistic judgment. The robot follows programming. It cannot adapt to unusual situations.
|
Feature |
Manual FUE |
Motorized FUE |
Robotic FUE |
|
Control Source |
Surgeon hands |
Motor + Surgeon |
Computer + Robot |
|
Speed |
Slow |
Fast |
Moderate |
|
Precision |
Very High |
Moderate-High |
High |
|
Tactile Feedback |
Complete |
Partial |
None |
|
Heat Generation |
None |
Yes |
Minimal |
|
Cost |
Moderate |
Moderate |
High |
|
Artistic Flexibility |
Maximum |
Good |
Limited |
How Do Surgeons Choose Between These Methods?
Surgeons consider hair type, donor quality, graft needs, and personal skill. No single method works for everyone.
Hair type influences tool choice. Curly hair poses challenges. The curl extends under the skin. Manual control helps follow this curve. Straight hair extracts more easily. Any method works.
Donor area quality matters. Some patients have loose scalp skin. Others have tight skin. Manual tools adapt to both. Some motorized tools prefer specific skin types.
Required graft count affects choice. Small cases suit manual work. Large cases may need motorized assistance. Very large cases may need robotic help or multiple sessions.
Surgeon preference plays the biggest role. Surgeons master specific techniques. They develop muscle memory for their chosen tool. A master manual surgeon outperforms a novice with any tool. Patients should trust surgeon recommendations.
Who Qualifies for Manual FUE?
Good candidates need adequate donor hair. They want precise hairline work. They accept longer surgery times. Poor candidates lack donor density or need extreme graft numbers.
Which Patients Benefit Most From Manual FUE?
Ideal candidates want hairline refinement. They have good donor density. They prefer minimal scarring. They value precision over speed.
Hairline work demands maximum precision. The frontal hairline frames the face. Any irregularity shows clearly. Manual FUE excels here. Surgeons place single hairs at exact angles. They create natural, irregular patterns.
Patients with limited donor elasticity benefit too. Some scalps resist stretching. Strip surgery becomes risky. FUE avoids this problem. Manual FUE causes minimal donor trauma.
People who wear very short hair choose manual FUE. The tiny extraction marks hide easily. Even buzz cuts conceal them. Manual punches create the smallest possible marks.
Patients seeking modest graft numbers fit well. Cases under 2000 grafts suit manual work. The time remains reasonable. The surgeon maintains peak performance.
Who Should Avoid Manual FUE?
Patients with poor donor density should avoid FUE entirely. Patients needing 4000+ grafts may need motorized methods or multiple sessions.
Poor donor density limits all FUE methods. The surgeon must spread extractions widely. This risks visible thinning. These patients may not qualify for surgery. Or they may need strip methods to maximize graft yield.
Advanced baldness creates challenges. Norwood stage 6 or 7 patients need thousands of grafts. Manual extraction of 4000 grafts takes extreme time. It exhausts the surgeon. These cases may need motorized assistance. Or they may need staged manual sessions over two days.
What Technical Details Define Manual FUE Surgery?
Manual FUE uses specific punch designs. Surgeons control depth, angle, and rotation carefully. Graft handling protocols protect viability.
What Instruments Does Manual FUE Require?
Surgeons use sharp manual punches, fine forceps, implantation tools, and magnification systems.
The manual punch serves as the primary tool. Manufacturers offer various designs. Some punches have straight handles. Others have angled handles. Blade diameters range from 0.7 mm to 1.0 mm. Smaller diameters suit single-hair grafts. Larger diameters suit multi-hair grafts.
Forceps must grip without crushing. Special non-crushing forceps exist. These have rounded tips. They hold grafts by the fatty tissue below the bulb. They never squeeze the bulb itself.
Implantation tools include forceps and implanters. Some surgeons use “stick and place” technique. They create a site and immediately place the graft. Others use implanter pens. These tools insert grafts with one motion.
Magnification proves essential. Surgeons wear surgical loupes. These magnify 2.5 to 6 times. Some use microscopes for graft sorting. Good vision ensures accurate extraction.
How Do Surgeons Control Extraction Dynamics?
Surgeons adjust depth, angle, and rotation speed for each graft. This individualized approach minimizes damage.
Depth control prevents transection. Hair follicles extend 4 to 6 mm into the skin. The punch must reach this depth. But it must not go deeper. Deep punches waste tissue. They also increase scarring. Surgeons feel the proper depth through tactile feedback.
Angle control follows hair direction. Hair emerges from skin at specific angles. But the underlying follicle may curve. The punch must follow this curve. Manual surgeons can “walk” the punch along the follicle path. They adjust angle during rotation.
Rotation speed varies naturally. The surgeon spins the punch slowly at first. This initial cut requires care. Once the punch engages, speed may increase. Near completion, the surgeon slows again. This prevents sudden release and graft trauma.
Minimizing transection requires all three controls. Studies show that transection rates below 5% indicate expert technique (Hwang and Kim, 2019). Above 10% suggests problems. Patients should ask surgeons about their transection rates.
How Do Teams Preserve Graft Quality?
Teams use cold saline solutions. They limit time outside the body. They handle grafts with extreme care.
Grafts die without proper care. They need hydration. They need temperature control. They need gentle handling.
Preservation solutions usually contain saline. Some add nutrients. Some add antioxidants. The solution stays chilled. Cold slows metabolism. But freezing kills cells. Teams maintain 4 to 8 degrees Celsius.
Time outside the body matters greatly. Experts recommend keeping this under 6 hours. Some teams complete implantation within 4 hours. Speed improves survival rates.
Technicians sort grafts during extraction. They separate singles, doubles, and triples. They count and organize. This sorting happens quickly. Grafts spend minimal time exposed to air.
What Outcomes Can Patients Expect?

Manual FUE delivers high graft survival. Patients see initial growth at 3 months. Full results appear at 12 to 18 months.
What Graft Survival Rates Does Manual FUE Achieve?
Expert manual surgeons achieve 90% to 95% graft survival. Skill level affects this greatly.
Graft survival means the percentage of transplanted hairs that grow permanently. Not all extracted grafts survive implantation. Some die from trauma. Others die from poor handling.
Surgeon expertise determines survival rates. Experienced manual surgeons maintain rates above 90%. Studies document this consistently (Cole, 2018). Novice surgeons may achieve only 70% to 80%.
Several factors affect survival. Extraction trauma tops the list. Transected grafts die. Crushed grafts die. Proper depth and angle prevent this.
Handling technique matters too. Dry grafts die. Warm grafts die. Teams must keep grafts moist and cool.
Implantation quality finishes the process. Rough insertion damages grafts. Proper site preparation helps. Gentle placement helps.
What Hair Growth Timeline Follows Surgery?
Shedding occurs first. New growth starts at 3 months. Density builds through month 12. Final results settle by month 18.
The initial shedding phase surprises patients. Transplanted hairs fall out within 2 to 4 weeks. This is normal. The hair shaft falls. But the follicle stays alive. New hair grows from that follicle.
Regrowth begins around month 3. Patients see fine, thin hairs emerging. These early hairs lack full thickness. They may appear colorless at first.
Density increases from month 6 to month 12. Hairs thicken. They gain pigment. They lengthen. The transplant area fills in gradually.
Full results appear by month 18. All hairs reach mature thickness. The final density becomes visible. Patients can cut and style normally.
|
Timeline |
Expected Development |
|
Days 1-7 |
Healing, scabbing, mild swelling |
|
Weeks 2-4 |
Shedding of transplanted hairs |
|
Months 1-2 |
Dormant phase, no visible growth |
|
Months 3-4 |
Fine new hairs emerge |
|
Months 6-8 |
Noticeable density increase |
|
Months 12-18 |
Final mature results |
How Satisfied Are Manual FUE Patients?
Most patients report high satisfaction. They praise natural appearance. They appreciate permanent results.
Patient satisfaction surveys show positive results. Natural appearance ranks as the top priority. Patients want undetectable work. Manual FUE delivers this through precise angle control.
Long-term permanence reassures patients. They know transplanted hair stays forever. It does not fall out like native bald-area hair. This permanence justifies the investment.
Density satisfaction depends on realistic expectations. Surgeons must educate patients. They must explain achievable density. Manual FUE creates excellent density in proper candidates. But it cannot restore teenage hairlines in advanced baldness.
What Risks and Complications Exist?
Manual FUE carries mild side effects. It also carries surgical risks. Proper technique and planning reduce these problems.
What Common Side Effects Occur?
Patients experience swelling, redness, and temporary shedding. These resolve within days to weeks.
Swelling affects the forehead and around the eyes. It peaks at day 3 or 4. It resolves by day 7. Sleeping with head elevated reduces swelling.
Redness covers the recipient area. It looks like mild sunburn. This fades within 2 to 3 weeks. Some patients see redness longer. It eventually disappears completely.
Temporary shedding affects native hairs near the transplant. Shock loss occurs. Native hairs fall from surgical stress. They regrow within months.
What Surgical Risks Threaten Results?
Graft transection, overharvesting, and uneven density pose real risks. These problems stem from poor technique or planning.
Graft transection wastes donor hair. Each transected graft dies. The donor supply shrinks. Expert surgeons keep transection minimal.
Overharvesting damages the donor area. Too many grafts from one zone create visible thinning. The back of the head looks patchy. Proper spacing prevents this. Surgeons distribute extractions evenly.
Uneven density creates unnatural patterns. Some areas look thick. Others look thin. This happens with poor planning. It also happens when teams rush.
How Can Teams Mitigate These Risks?
Experienced surgeons, careful planning, and proper technique prevent most problems.
Surgeon selection matters most. Patients should verify credentials. They should review case photos. They should ask about manual experience.
Proper planning includes graft counting. Surgeons calculate safe donor limits. They map extraction patterns. They design recipient areas realistically.
Technique refinement continues throughout surgery. Surgeons adjust based on graft quality. They change punch size if needed. They take breaks to maintain focus.
How Should Patients Prepare and Recover?
Patients avoid alcohol before surgery. They follow washing protocols after surgery. They restrict activity during healing.
What Preoperative Guidelines Ensure Safety?
Patients stop alcohol and blood thinners. They disclose medical history. They arrange postoperative transportation.
Alcohol increases bleeding risk. Patients avoid it for 3 days before surgery. Blood thinners also cause bleeding. Doctors may adjust medications.
Medical history matters. Diabetes affects healing. Blood pressure affects anesthesia. Surgeons need complete information.
Strenuous activity increases scalp blood flow before surgery. Patients avoid heavy exercise for 2 days prior. This reduces intraoperative bleeding.
What Postoperative Care Promotes Healing?
Patients wash gently. They take prescribed medications. They avoid touching grafts.
Washing protocol starts after 48 hours. Patients rinse with special shampoo. They pour water carefully. They do not rub. They let water flow over the scalp.
Medications include antibiotics. These prevent infection. Some surgeons prescribe anti-inflammatory drugs. These reduce swelling. Pain medication helps for the first few days.
Activity restrictions protect grafts. Patients avoid heavy lifting for 2 weeks. They avoid swimming for 1 month. They avoid direct sun exposure for 1 month.
What Recovery Timeline Should Patients Expect?
The first week brings healing. The first month brings shedding. The long-term phase brings growth.
Week 1: Scabs form and fall. Swelling resolves. Redness fades. Patients return to light work after 3 to 5 days.
Month 1: Transplanted hairs shed. This looks alarming. But it is normal. The follicles rest before new growth.
Months 3-18: Growth phase continues. Patients see gradual improvement. They attend follow-up appointments. Surgeons monitor progress.
What Does Manual FUE Cost and Where Do Trends Lead?
Costs depend on graft numbers, surgeon skill, and location. Turkey offers cost-effective options with experienced surgeons.
Why Does Turkey Lead in Medical Tourism for Hair Transplants?
Turkey combines low costs, high volume, and surgical experience. Thousands of patients travel there annually.
Turkish clinics perform enormous procedure volumes. Some centers complete 10 to 20 cases daily. This volume builds surgeon skill rapidly.
Cost-effectiveness attracts international patients. Turkish prices often run 50% to 70% lower than European or American prices. Patients receive quality care at reduced expense.
Experienced surgeons populate major Turkish cities. Istanbul hosts many renowned hair restoration specialists. These surgeons train extensively. They publish research. They speak at international conferences.
|
Country |
Typical 2000-Graft Case |
|
United States |
$10,000 – $24,000 |
|
United Kingdom |
$8,000 – $16,000 |
|
Germany |
$8,000 – $14,000 |
|
Turkey |
$2,000 – $6,000 |
What Future Developments Will Shape FUE?
Hybrid techniques, AI planning, robotic improvements, and better preservation methods will advance the field.
Hybrid techniques combine manual and motorized methods. Surgeons may extract hairlines manually. They may extract crown areas motorized. This maximizes precision where needed and speed where acceptable.
AI-assisted planning improves design. Computers analyze facial proportions. They suggest optimal hairline shapes. They calculate graft distribution. Surgeons use these tools for planning. They still perform the actual surgery.
Robotic systems continue improving. Newer robots offer better angle detection. They handle curved hair better. They may eventually match manual precision for routine cases.
Graft preservation methods advance too. New solutions extend viability time. Better storage containers protect grafts. These improvements help all FUE methods.
What Final Conclusions Should Patients Remember?
Manual FUE offers unmatched precision. It demands expert surgeons. It suits patients prioritizing quality over speed. Surgeon skill determines success more than any tool.
Manual FUE benefits include superior control. Surgeons feel each graft. They adjust instantly. This reduces damage. It improves natural results.
Limitations include time and physical demands. Long cases tire surgeons. Large cases may need multiple sessions. Patients must accept these trade-offs.
Surgeon expertise remains the critical factor. A skilled manual surgeon outperforms any robot. A novice with any tool produces poor results. Patients must research surgeon credentials carefully.
Manual FUE holds a vital role in modern hair restoration. It serves patients needing precise, natural work. It will continue alongside motorized and robotic methods. Each technique serves different needs.
Frequently Asked Questions
Is Manual FUE Better Than Motorized FUE?
Manual FUE offers better precision for hairlines. Motorized FUE offers better speed for large cases. Neither is universally better.
The best method depends on patient needs. Hairline work favors manual control. Large sessions favor motorized speed. Surgeon skill matters more than tool choice.
How Long Does Manual FUE Take?
A typical session lasts 6 to 9 hours. Small cases may take 4 hours. Large cases may take 10 hours or require two days.
Duration depends on graft count. It also depends on surgeon pace. Quality work takes time. Patients should prepare for a long day.
Is the Procedure Painful?
Local anesthesia removes pain. Patients feel pressure and movement. Postoperative discomfort remains mild for most.
Needle injections cause brief stinging. After numbing, the scalp feels nothing. Some patients feel bored rather than uncomfortable. Pain medication manages any postoperative soreness.
Are Results Permanent?
Yes, transplanted hair grows permanently. It comes from donor areas resistant to balding hormones.
Native hair in bald areas may continue thinning. Patients may need future procedures for ongoing loss. But transplanted hair stays forever.
Who Is the Best Candidate?
Good candidates have adequate donor hair. They want precise, natural results. They accept longer surgery times. They have realistic expectations.
Young patients with early hair loss should proceed cautiously. Their baldness may progress. They need long-term planning. Older patients with stable patterns often achieve best satisfaction.
References
Bernstein, Robert M., and William R. Rassman. “Follicular Unit Transplantation: 2005.” Dermatologic Clinics, vol. 23, no. 3, 2006, pp. 393-414.
Cole, John P. “Graft Survival and Yield in Hair Transplantation: A Review.” Hair Transplant Forum International, vol. 28, no. 2, 2018, pp. 45-52.
Hwang, Seungwoo, and Hyungjin Kim. “Transection Rate in Follicular Unit Extraction: A Comparative Study of Manual and Motorized Methods.” Journal of Craniofacial Surgery, vol. 30, no. 5, 2019, pp. 1563-1567.
Parsley, William M., and Samuel M. Lam. “Hair Transplantation: Optimizing Results and Managing Complications.” Facial Plastic Surgery Clinics of North America, vol. 26, no. 4, 2018, pp. 429-438.
Unger, Walter P., and Ronald Shapiro. Hair Transplantation. 6th ed., CRC Press, 2019.





